Who gives the aged care facility permission to restrain you?
Should you add additional clauses to your Power of Guardianship or Medical Decision Maker document? Do you try and guess what you want done in the nursing home as far as being restrained goes? Or should you keep those powers out of your lifestyle and medical appointment until an actual restraint issue arises? This article works through that choice.
What is a lifestyle and medical decision appointment document?
On Legal Consolidated’s website, you build lifestyle and medical documents for every State and Territory. You give a person you trust the power to protect you. This is for your personal, lifestyle, accommodation and healthcare decisions. This is when you cannot make the decision yourself. Every State has its own name for such a document. For brevity, we call them in this article ‘lifestyle and medical appointments’.
| State or Territory | Document authorising someone to make lifestyle and medical decisions for you | Who you appoint |
| New South Wales, Tasmania and Western Australia | NSW: Appointment of Enduring Guardian. Tasmania: Enduring Guardianship. WA: Enduring Power of Guardianship. | Enduring Guardian |
| Australian Capital Territory and Queensland | The Enduring Power of Attorney also deals with lifestyle and medical decisions. See the Legal Consolidated Australian Capital Territory and Queensland documents. | Attorney |
| South Australia | Advance Care Directive | Substitute Decision Maker |
| Northern Territory | Advance Personal Plan | Decision Maker |
| Victoria | Enduring Power of Attorney for personal and lifestyle matters; Appointment of Medical Treatment Decision Maker for medical treatment | Medical Treatment Decision Maker |
On Legal Consolidated’s website you can build all 16 Australian financial and lifestyle/medical appointments. They are carefully drafted according to the State or Territory you select in the building process. This is so that they have the highest chance of being accepted by banks, titles offices, hospitals and nursing homes.
When does your aged care home want permission to restrain you?
Before deciding whether restraint powers belong in your lifestyle and medical appointment, consider why an aged care home asks for them. Dementia, delirium, brain injury, pain, fear and unfamiliar surroundings change how you behave. You may fall, wander into danger, strike another person or pull out medical equipment.
An aged care facility should not ignore a real danger to you, another resident or its staff. However, it should first look for safer and less restrictive ways to control you. From Legal Consolidated’s experience, restraint too often becomes the convenient answer before every better answer is exhausted.
What happens when you are of unsound mind?
When you cannot give consent, staff should ask your authorised Attorney, Guardian or Medical Treatment Decision Maker before controlling your movement, surroundings or medication. The law calls that control a ‘restrictive practice’.
Five ways you are restrained in aged care
Contentiously, and in a way many of our clients consider arbitrary, the Commonwealth Government has attempted to narrow restrictive practices to:
- Chemically restraining you: Staff give you a drug mainly to control your behaviour rather than treat an illness. A sedative used to keep you quiet is a restraint. The same drug used to treat a diagnosed condition is treatment. Why the drug is given matters.
- Restricting your environment: Staff stop you reaching a place or object. They lock a ward, garden or fridge, disable your electric wheelchair or put your walking frame out of reach. Some of our clients call it imprisonment.
- Mechanically restraining you: Staff use a device to limit your movement. This includes a lap belt, bedrail, restrictive chair or clothing that stops you moving freely.
- Physically restraining you: A human uses force against your will. Staff hold your arms, hold you down, block a doorway or steer you away from an exit.
- Isolating you: The legal label is ‘seclusion’. Staff keep you alone in a room or area that you cannot leave. A quiet room you choose is not seclusion. A room you are stopped from leaving can be.
These five categories appear in the Aged Care Act 2024 (Cth) ss 17–18 and the Aged Care Rules 2025 (Cth) r 17-5. They are likely to be reviewed in the future and potentially changed, especially as each State is starting to interpret the words differently. See the Office of Public Advocates published Research Essay:
Providers … are faced with uncertain rules regarding restrictive practises that are unnecessarily confusing. This includes inconsistent definitions between the State and Commonwealth as well as ambiguous authorisation requirements, both of which were evidenced in the decision of Re KF; Re ZT; Re WD [2019] SACAT 37.

Does your Power of Guardianship let your Decision Maker approve or refuse restraints?
Not necessarily.
Your lifestyle and medical appointment appoints an Attorney, Guardian or Medical Treatment Decision Maker. But the appointment does not itself approve any restraint. Nor does it always give your Decision Maker authority to approve or refuse one.
Each Australian State and Territory draws a different line. Some recognise the authority already held by your Decision Maker. Others require a specific function, a separate statutory appointment or a tribunal order. The differences are explained below.
Even where your Decision Maker has authority, consent is given when the actual restraint is proposed. The Decision Maker considers what is proposed, why it is needed, what alternatives were tried, how often it is used and how long it lasts.
A document signed years earlier does not answer those questions.
Does a legally prepared restraint clause solve the problem?
The following restraint clause was prepared by a lawyer who has practised in guardianship, aged care and substitute decision making for many years. Legal Consolidated does NOT recommend that you put restraint clauses in your document. But if you did, these are the kind of words you use:
Example of a Restraint Clause in a Power of Guardianship/ Decision Maker/ Enduring POA
In addition to the ordinary functions given by this appointment, I expressly give the function of giving or withholding informed consent to the use of a restrictive practice in relation to me, including chemical restraint, environmental restraint, mechanical restraint, physical restraint and seclusion.
Before giving consent, they must consider my wishes, preferences, rights and dignity and a written proposal identifying the practice, how it is to be used, its duration, frequency and intended outcome.
They must be satisfied on current clinical and behavioural evidence that the proposed practice is:
- permitted by the law applying when the decision is made;
- necessary and proportionate to an identified risk of harm and the least restrictive response available;
- proposed only after less restrictive alternatives have been considered or tried;
- used only as a last resort and for the shortest time necessary; and
- is monitored, reviewed, recorded and included in any Behaviour Support Plan required by law.
This and other attempted restraint clauses we have seen have fatal problems as set out below.
The problems with restraint clauses in lifestyle and medical appointments:
The Restraint Clause in the Medical Decision Maker/POG/POA gives authority, not consent
The above clause does not approve a locked door, drug, belt, physical hold or seclusion. The aged care facility still needs informed consent when the restraint is proposed. That consent deals with the actual restraint, including its duration, frequency and intended outcome under the Aged Care Rules 2025 (Cth) r 162-15.
The Restraint Clause unduly limits your Guardian/Attorney/Substitute Decision Maker/ Medical Treatment Decision Maker
In the above restraint clause, ‘must’ is another condition on your Guardian’s authority. Persuasive evidence may be given orally. The Behaviour Support Plan may be out of date. The meanings of “current”, “least restrictive” and “shortest time” are often disputed. The extra words give someone a reason to argue that your Guardian was not entitled to act.
Restraint Clauses in POGs/EPAs/Medical Decision maker are often misinterpreted
The same drug, locked door or device is treatment in one setting and restraint in another. Its legal character depends on why and how it is used. A private definition does not settle the medical facts or the meaning imposed by the law then in force.
The restraint clause relies on today’s law. The current five categories and the expression ‘Behaviour Support Plan’ come from the present Commonwealth aged care scheme. The appointment may be needed decades after it is signed. These new laws are likely to change from time to time, especially as they do not appropriately cover hospitals, disability services or private homes.
Restraint Clauses cannot create powers that belong to the tribunal
A restraint clause written into your document does not authorise detention, force or another power that legislation gives only to a court or tribunal. In The Public Advocate v C, B [2019] SASCFC 58, ordinary guardianship authority did not authorise a coded locked ward.
Restraint clauses make your appointment difficult to witness and accept
From what we are seeing these confusing Restraint Clauses are difficult to get witnessed. In NSW, in particular, the Courts are refusing to witness them. I do not blame them, the authorised witness must understand the extra function well enough to explain the appointment. Lawyers are also refusing to sign them on the same basis.

Although the NSW Local Court does not supervise Enduring Guardians, it is quick to state what they may and may not do. Its guidance that treatment must ‘promote or maintain’ your health and wellbeing helps explain why Legal Consolidated is seeing Local Court Registrars refuse to witness appointments containing added restraint clauses.
The nursing facility challenges Restraint Clauses it does not like
The aged care home, doctor and lawyer must decide what the added restraint clauses mean. From our experience, the aged care facility often rejects the restraint clause requiring a legal opinion and then a trip to the tribunal. This is especially the case if the aged care facility does not like the direction your Restraint Clause is taking.
Attempting to define a restraint power restricts that power
Every attempt to define the restraint power curtails it. The clause does not replace the consent required when the actual restraint is proposed. Nor does it override the State or Territory law then in force. Best practice requires that the principal lifestyle and medical appointment should remain broad, conventional and recognisable. It should not contain exotic clauses such as restraint wording. Legal Consolidated follows that best practice.
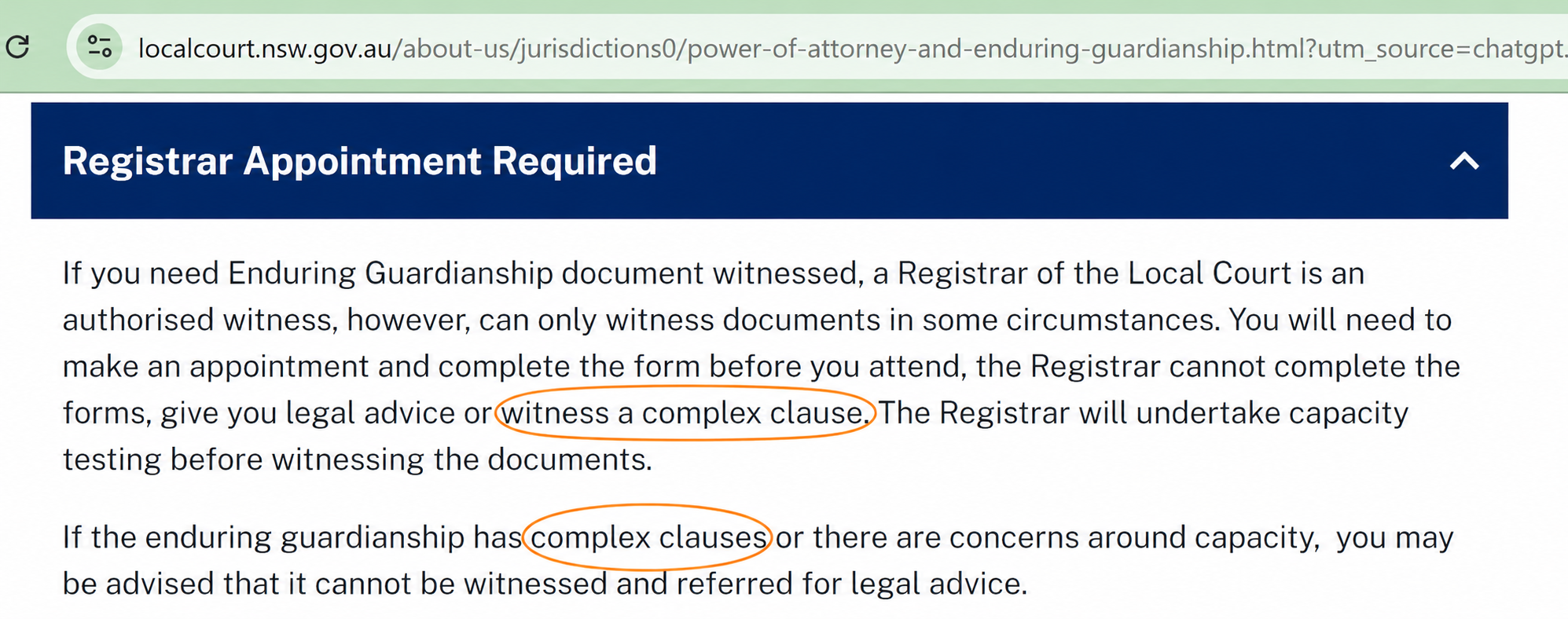
Even Local Court Registrars authorised by law to witness Enduring Guardianships look for the exit when they see a complex restraint clause.
Why are ‘ordinary’ restraint words in your document dangerous?
You may use a word. Someone else may believe that word means something different. Court decisions are riddled with ordinary words that were so misunderstood that a judge had to decide what they meant. Time makes the problem worse. Language, medicine and legislation move after you sign. Consider these examples of everyday words that were used in Wills:
What does ‘all my belongings’ mean?
A man aged 27 left a handwritten suicide note to his mother:
‘All my belongings I give to you.’
Did ‘belongings’ mean only his clothes and other physical items? Or did it include cash, shares, wages owed, a tax refund, superannuation death benefits and insurance money paid to his estate? After much deliberation, the Court decided that it meant his entire estate: Public Trustee v Alexander – Estate of Alexander [2008] NSWSC 1272, [26]–[40].
Does a Mercedes-Benz form part of ‘personal effects’?
A Will gave his wife his ‘personal effects’. Did that include the $60,000 Mercedes-Benz? Did it include cash, bank deposits, shares and company notes? The Court decided that the Mercedes-Benz was a physical item he personally used. The money and investments were not: Lowe v Lowe [2015] NSWSC 48, [6]–[25], [32]–[33].
Does the word ‘use’ mean I can live in the dead person’s house?
A Will allowed the Executors to ‘use’ a house for two years without paying rent. Did that mean they could live there alone and force the stepson out? No. The Court decided that ‘use’ did not mean exclusive possession. The stepson could remain while the Executors accessed the property to archive, catalogue and sell the dead man’s artwork: Re Prior; Niran v Prior [2022] VSC 31, [31]–[48].
Who protected the man with dementia locked inside an aged care ward?
A man with dementia was locked in his ward. The Public Advocate had been appointed as his limited guardian for ‘accommodation and lifestyle’ and was happy to approve the confinement. Thankfully, the South Australian Full Court held that this ordinary guardianship authority did not authorise his detention. Rather, authority under s 32 had to be obtained from the Tribunal: The Public Advocate v C, B [2019] SASCFC 58, [1]–[5], [64], [76]–[77]. A private clause cannot manufacture a power that legislation gives to a court or tribunal. The South Australian Office of the Public Advocate explains the need for that special order.
The lesson is blunt. Even a Tribunal-appointed guardian could not turn a locked door into lawful care. A private restraint clause cannot create a power that legislation gives only to a court or tribunal. Nor can words signed years earlier predict whether the Tribunal will grant that authority when the real facts arise.
Can the legal meaning of a ‘cage’ change?
In 2014, the United Kingdom Supreme Court used one clear test for a deprivation of liberty. Lady Hale wrote:
‘A gilded cage is still a cage.’
Twelve years later, the same Court overruled that test. It held that confinement instead requires a practical assessment of the type, duration, effects and manner of the restriction. See P v Cheshire West and Chester Council [2014] UKSC 19, [46]; A Reference by the Attorney General for Northern Ireland [2026] UKSC 16, [53], [183]–[185]. These two decisions do not state Australian law. But they show why a private restraint clause drafted today is a poor predictor of tomorrow’s law and medicine.
If ‘belongings’, ‘personal effects’, ‘use’ and even a legal test for confinement change with context and time, ‘restraint’, ‘seclusion’ and ‘emergency’ do not become safe when pasted into your Power of Guardianship/Decision Maker document.
How do Australian State and Territory restraint laws differ?
Australia has no national rule. The document names may look similar, but the powers are not.
- NSW, Tasmania and Western Australia: Enduring Guardians. NSW requires a specific restraint function. Tasmania starts with broader personal authority. Western Australia looks for plenary authority or an express limited power.
- The Australian Capital Territory and Queensland: Enduring Powers of Attorney. The ACT gives general personal and healthcare powers. In EJ [2026] QCAT 175, a Queensland Attorney can consent in residential aged care.
- South Australia: Advance Care Directive. Detention or force requires the Tribunal.
- Northern Territory: Advance Personal Plan. But its Decision Maker ordinarily cannot consent to restraints.
- Victoria. A separate restrictive practices nomination is required
Why is a tribunal better than restraint clauses in your POG or EPA?
A tribunal examines the actual restraint, current evidence, available alternatives and the law and medicine then in force.
In Hunter (a pseudonym) [2025] NSWCATGD 25, NCAT reviewed a current guardianship order. It considered medication given when needed, known as ‘PRN’ medication, and restricted access to sharp objects and chemicals. Restraint was limited to a last resort under a Behaviour Support Plan that required regular review.
Although Hunter concerned disability support of a 25 year old, the lesson applies. A tribunal considers the real person and current facts. An old restraint clause cannot do that. And for those that are a bit rusty on their Latin, ‘PRN’ is medication given when needed. It is from the Latin pro re nata.
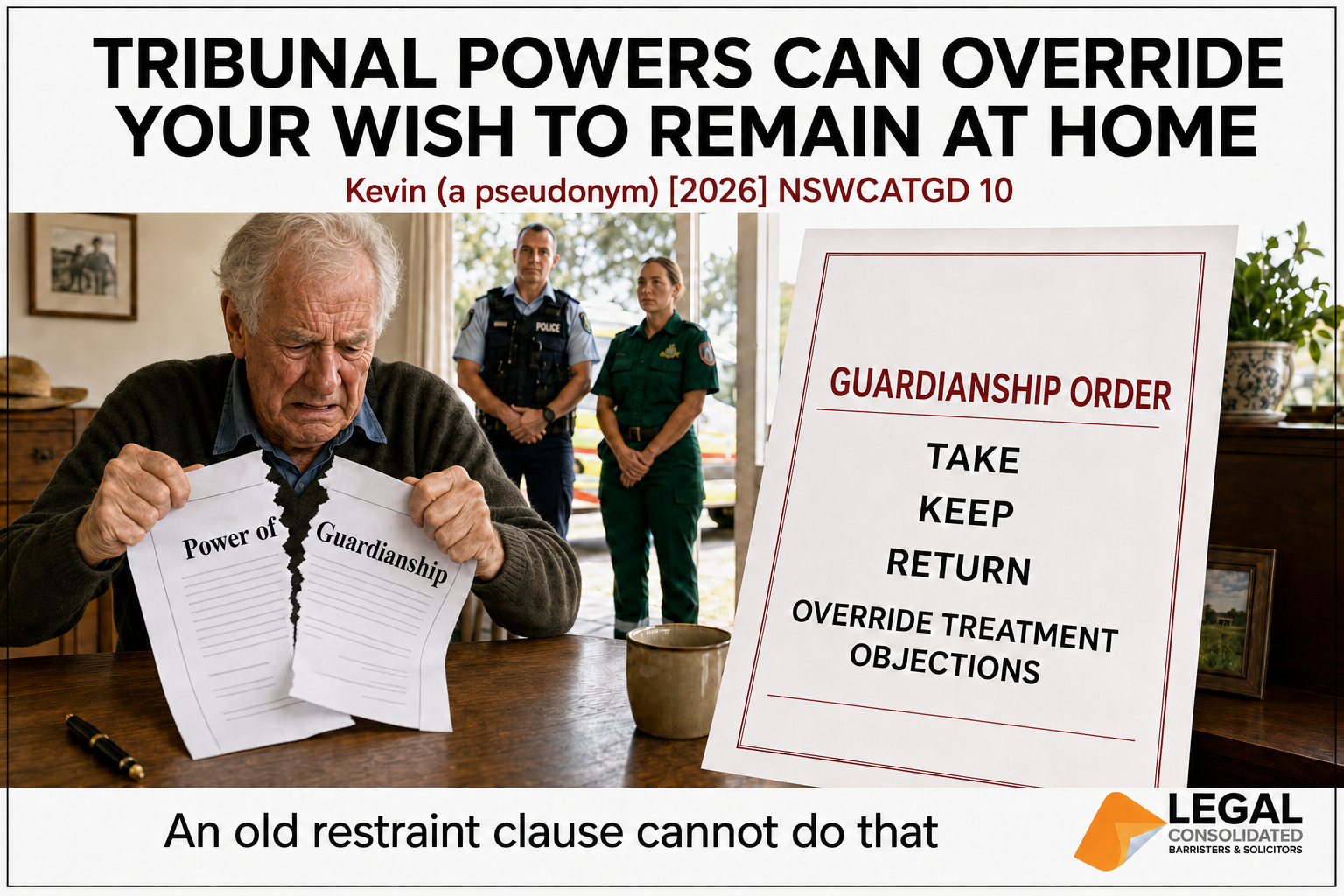
If the Tribunal can override your wish to remain at home, why damage your Power of Guardianship with a restraint?
Kevin (a pseudonym) [2026] NSWCATGD 10 makes the point clearly. Kevin was an 80-year-old man living alone on his farm. With no ‘formal diagnosis of a disability’ (paragraph 16), the NSW Civil and Administrative Tribunal (NCAT) gave his guardian power to authorise police and ambulance officers to take him to an approved place, keep him there and return him if he escaped. NCAT authorised the guardian to override Kevin’s objections to major or minor medical treatment.
Kevin did not concern restrictive practices in residential aged care. But it shows the limited value of restraint wording signed years earlier. The Tribunal considers your wishes, but decides the issue using the actual facts, medical evidence and law then in force. It identifies the precise powers required and the conditions applying to them.
Why damage your Power of Guardianship with an old restraint clause that does not bind the Tribunal and cannot perform that current assessment?
Do not contaminate your Power of Guardianship with restraint clauses
From what Legal Consolidated sees in practice, added restraint clauses do not work. They make the appointment harder to understand, witness and accept. They restrict ordinary powers, make the document unusable for other purposes and invite a challenge. Just do not add them.
Legal Consolidated does not contaminate your Power of Guardianship, Enduring Power of Attorney or Medical Treatment Decision Maker appointment with restraint clauses.
Your Attorney, Guardian or Medical Treatment Decision Maker remains bound by the legislation, your wishes and values, the least restrictive approach and any decision reserved to a court or tribunal. The aged care home remains bound by Commonwealth law. Attempts to address those matters with added clauses cause problems.

This article was co-authored by Adjunct Professor Dr Brett Davies and Chivy Chan, a law graduate of the University of Staffordshire in Stoke-on-Trent, England. She is currently completing Practical Legal Training with the Institute of Legal Training.
Legal Consolidated Power of Attorney documents and guides
Financial Powers of Attorney
Build for your State or Territory:
NSW · VIC · QLD · WA · SA · TAS · ACT · NT
Questions about your financial Power of Attorney:
- Can a Power of Attorney be used to steal my money?
- Can my Attorney act as Trustee of my trust?
- Can my Attorney change my superannuation binding nomination?
- Can my financial planner witness my Power of Attorney?
- Can I sign a Power of Attorney if I lack mental capacity?
- Does my Power of Attorney work outside its home State?
- Should I add more clauses to my Power of Attorney?
- Do all Attorneys need to accept their appointment now?
Lifestyle and medical appointments
Build for your State or Territory:
NSW · QLD · WA · SA · TAS · ACT · NT
Victoria: appoint a Medical Treatment Decision Maker
Company Power of Attorney
Protect your company when a director goes missing, loses capacity or dies.
Australian authorities on Restraint Clauses in Power of Attorney/Power of Guardianship and Decision Maker documents
| • Aged Care Act 2024 (Cth) ss 17–18, 162–163. | • Australian Government Department of Health, Disability and Ageing, Consent for Restrictive Practices: Frequently Asked Questions (February 2026). |
| • Aged Care Rules 2025 (Cth) rr 6-20, 17-5, 162-5–162-75.
The hierarchy in r 6-20 is an interim Commonwealth measure. It operated until 1 December 2026 while the States and Territories develop their own consent and guardianship arrangements. However, the end of that hierarchy does not end the Commonwealth rules governing restrictive practices. It changes who has authority to provide the required consent. |
• Powers of Attorney Act 2006 (ACT) s 13. |
| • Guardianship Act 1987 (NSW) s 6E. | • New South Wales Civil and Administrative Tribunal, Restrictive Practices and Guardianship (Fact Sheet, June 2024). |
| • Public Trustee v Alexander – Estate of Alexander [2008] NSWSC 1272, [26]–[40]. | • Health Care Decision Making Act 2023 (NT) s 29. |
| • Lowe v Lowe [2015] NSWSC 48, [6]–[25], [32]–[33]. | • Northern Territory Public Guardian and Trustee, ‘Information for health care decision makers’. |
| • Re Prior; Niran v Prior [2022] VSC 31, [31]–[48]. | • Queensland Civil and Administrative Tribunal, Aged Care: Restrictive Practices (Frequently Asked Questions, July 2026). |
| • The Public Advocate v C, B [2019] SASCFC 58, [1]–[5], [64], [76]–[77]. | • South Australian Office of the Public Advocate, ‘Restrictive practices’. |
| • P v Cheshire West and Chester Council [2014] UKSC 19, [46]. | • Guardianship and Administration Act 1995 (Tas) (current compilation). |
| • A Reference by the Attorney General for Northern Ireland [2026] UKSC 16, [53], [183]–[185]. | • Victorian Department of Health, ‘Substitute decision-making and restrictive practices in residential aged care’ (20 November 2025). |
| • Hunter (a pseudonym) [2025] NSWCATGD 25. | • Western Australian Office of the Public Advocate, Restrictive Practices in Aged Care (Position Statement, July 2026). |